

Understanding Your Fertility Hormone Cycle: The HPOU Axis
What is the HPOU axis?
The HPOU Axis is the hormonal pathway between your brain (the Hypothalamus and Pituitary glands), your Ovaries, and your Uterus. The interaction and fluctuations of these hormones are what drives your menstrual cycle by promoting and regulating follicular development, ovulation, endometrial thickening, receptivity and release of your lining, and early embryonic development. It’s what I like to call your Fertility Hormone Cycle.
An Overview of The Fertility Hormone Cycle

All fertility pathologies result from disruption or dysregulation of this hormone cycle
Disruptions to this hormone cycle can be and often are the result of multiple factors including dysregulated immune function and inflammation, impaired digestion and fluid metabolism, exposure to household and environmental toxins, the effects of chronic stress, poor blood circulation, and/or nutritional deficiencies.
My job as a fertility specialist is to help you identify and unravel the potential disruptors and develop new perspectives and habits that actively promote fertility and overall health for you and your future baby.
The Optimized Cycle
An optimized fertility hormone cycle is the foundation of fertility and is observable in the characteristics of your menstrual cycle. The key characteristics of an optimized fertility/menstrual cycle are as follows:
Regularity
A regular cycle is a period that arrives at roughly the same interval month to month.
Cycle Length
An optimized cycle will arrive every 28 days, +/- a day or two. Cycle length is determined by both the length of your follicular phase — the window of time that begins with the first day of your period and ends with ovulation, and the length of your luteal phase — the window of time between ovulation and when your next period starts.
Moderate Flow
In an optimized cycle, the period flow will last about 4-5 days and is neither heavy nor scanty.
The volume and consistency (in term of thickness or thinness) of your period is a reflection of the thickness and vascularity of your uterine lining.
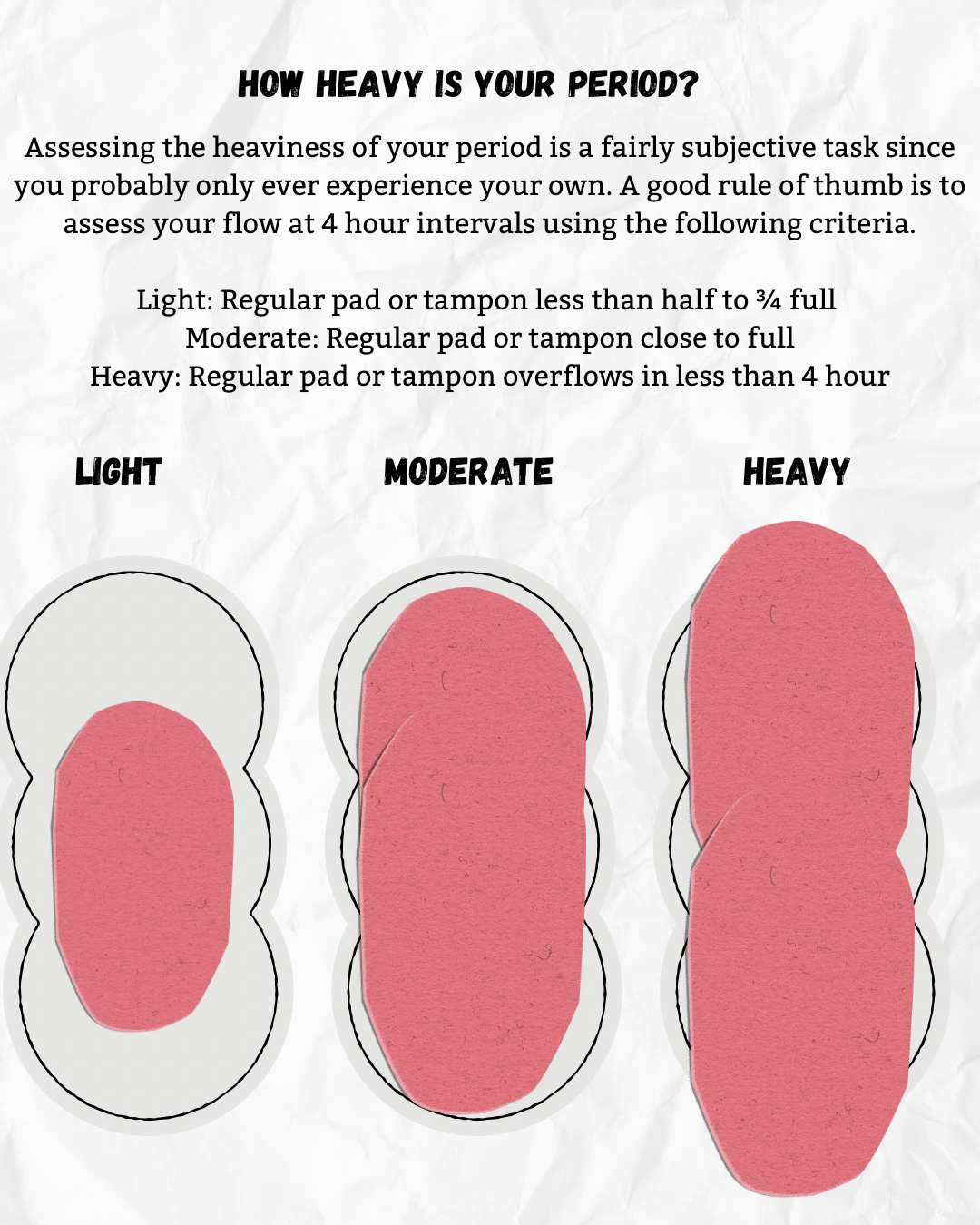
Evaluating Your Flow
For the sake of clear assessment and record keeping, the following is a guideline for assessing the heaviness of your period.
Moderate flow is filling a regular pad or tampon in about 4 hours without overflow
Heavy flow is overflowing a regular pad or tampon in less than 4 hours
Light or scanty is flow that doesn’t come close to saturating a regular pad or tampon in 4 hours
Fresh Red Flow
An optimized period will consist of primarily fresh, red blood with minimal clots, no pain or other typical PMS signs. Darker or lighter blood, the presence of clots or mucus, and blood that is either very thick or very thin/watery are all indicative of various patterns that can impact your fertility.
Cervical Fluid
In the days leading up to ovulation in an optimized cycle, there will be the obvious presence of clear, slippery, stretchy cervical fluid indicating rising estrogen levels as your ovarian follicles mature.
This cervical fluid plays a crucial role in facilitating the travel and survival of sperm from your vagina to your fallopian tubes.
A 14 day luteal phase
In an optimized cycle, the vacant follicle left behind after ovulation will quickly transform into the corpus luteum which will produce enough progesterone to prepare the uterine lining for implantation and to sustain early pregnancy until the placenta forms at around 10 weeks.
Sufficient progesterone levels are indicated by:
A 14 day luteal phase and no spotting before the period
A swift, significant, and sustained temperature rise following ovulation when charting BBT
Confirmation via inito/Mira of rising PdG levels (greater than 10 7dpo)
How to Read Your Cycle
Learning to track and interpret your period is important for diagnostic purposes and as a way to track changes to your fertility cycle as you move through your treatment plan and the four stages.
If you’re struggling with getting or staying pregnant, then your cycle is most likely not going to match an optimized cycle template.
The value of understanding what an optimized cycle looks like is in seeing where your cycle doesn’t line up with the template and then looking for clues into why you’re not matching up.
Cycle Day 1
Cycle day one is the first day of your period.
Emotionally and intuitively it often feels like your period is the end of your cycle, but according to standard medical convention, the first day of bleeding, not including spotting, is considered the first day of a new hormone cycle and so we call this Cycle Day (CD) 1.
Ovulation
Ovulation occurs 14 days prior to CD 1 in an optimized cycle. To calculate when you ovulated you subtract 14 days from your total cycle length.
For example, in the stereotypical 28 day cycle, you would subtract 14 from 28 and assume that ovulation occurred on cycle day 14.
However, if you have a cycle that is longer or shorter than 28 days, your ovulation day will not fall on cycle day 14. In a 30 day, ovulation would likely occur on CD 17, and in a 26 day cycle, ovulation would likely be occurring on day 12.
As you can see, relying on math alone is problematic. Ovulation day will shift depending on how you count the days and whether you use simple subtraction or count the actual days on a calendar like in the example below.
To truly identify ovulation you will need to use multiple methods of observation.
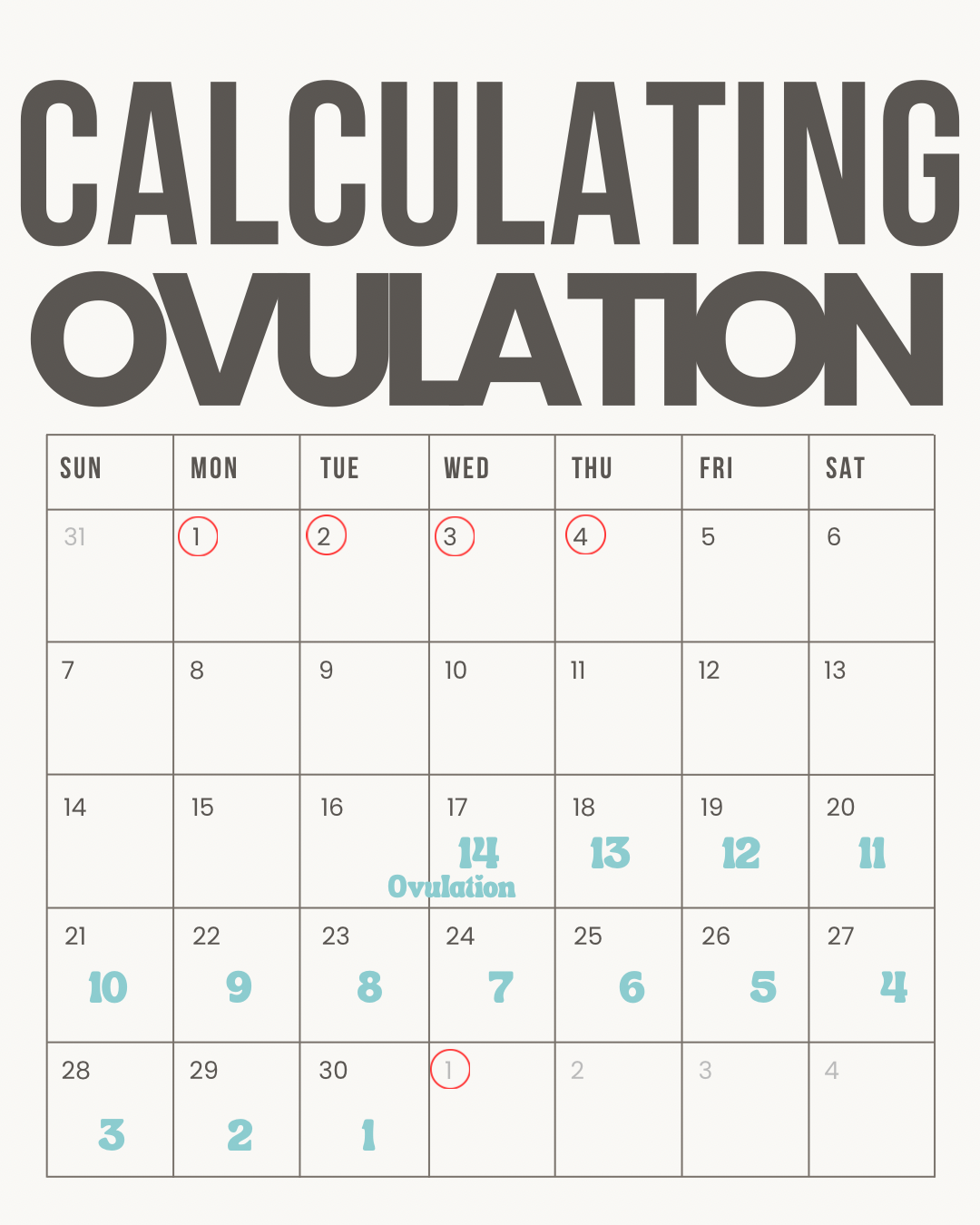
In this example CD 1 is on the first of the month, followed by 3 more days of bleeding (4 day bleed).
The next period started on the first of the following month which gives a total cycle length if 30 days.
Counting back 14 days before the next period puts ovulation at approximately day 17.
It’s important to keep in mind that using math alone to try to pinpoint when your ovulation occurs is never the primary way you want to confirm ovulation.
We’re just using this general model to illustrate what an optimized cycle typically looks like.
Using the calendar alone you’re doing a lot of analyzing in hindsight. It’s a good way to track what happened, but not an effective tool for predicting what’s going to happen.
This hormone cycle can very easily be thrown off by a multitude of factors including stress, medication, travel, etc., so it’s important to track other indicators of ovulation such as your cervical fluid changes, inito or Mira data, and BBT (which is also more of a confirmation metric than a predictor, but provides diagnostically significant information from an Eastern Medicine perspective).
Total Cycle Length
Total Cycle Length is the number of days from the first day of your period (spotting not included) to the day before your next period starts.
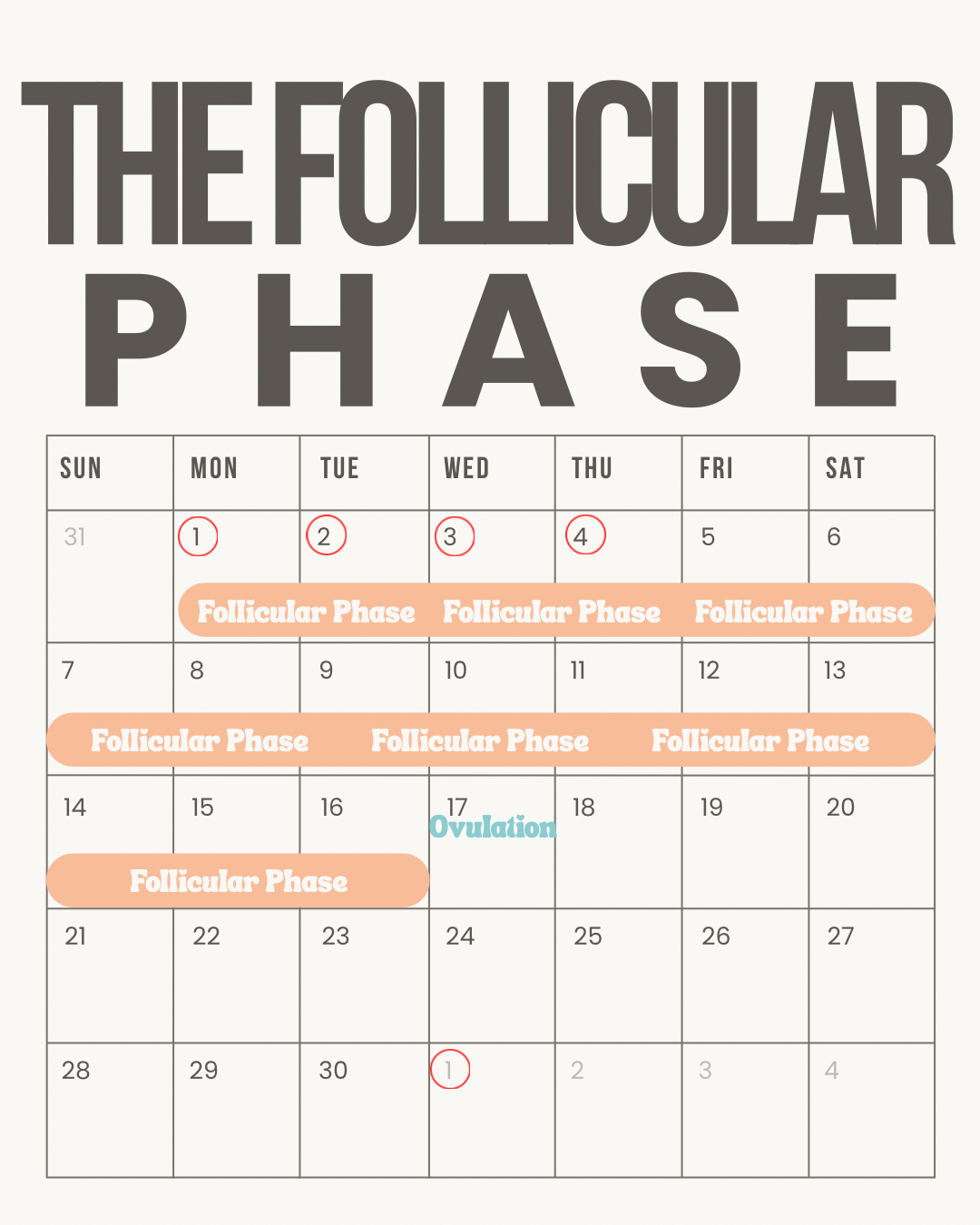
Determining Follicular Phase Length
The Follicular Phase is where the length of your cycle can vary. The length of your follicular phase is determined by how long it takes your body to go from CD 1 (first day of your period) to ovulation.
There are many factors that can influence this process including impaired receptivity of the follicles to FSH, impaired pituitary production of FSH, impaired estrogen feedback to the pituitary, insulin resistance, and chronic inflammation.
Supporting proper hormone signaling and responsiveness in the follicular phase is vital to ensuring optimal egg quality, proper corpus luteum formation, and progesterone production sufficient to stabilize your uterine lining and sustain early embryo development.
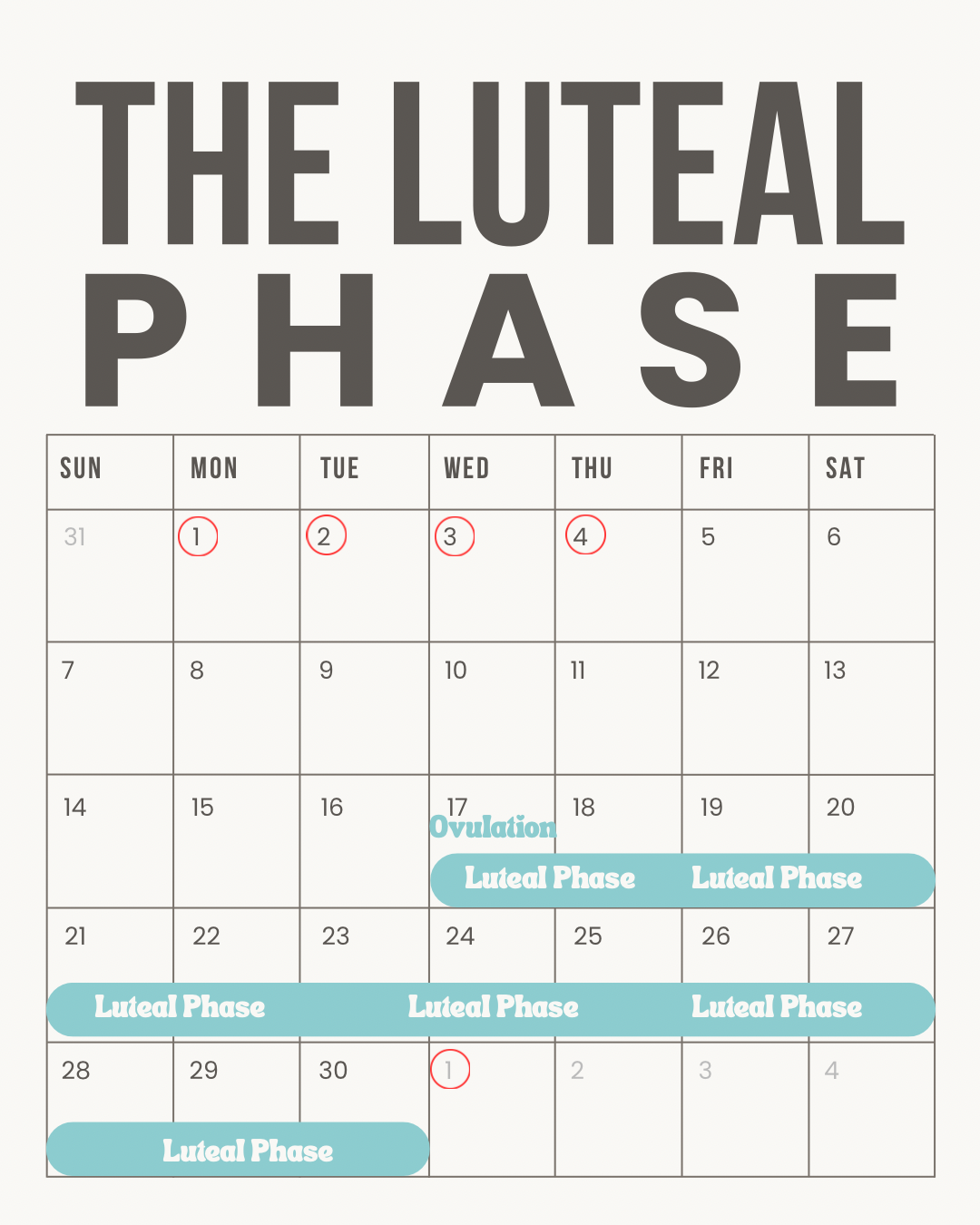
Determining the Length of Your Luteal Phase
Your Luteal Phase is the time between ovulation and your subsequent period. In an optimized cycle, the luteal phase is always 12-14 days. If your luteal phase is not consistently lasting 12-14 days, that can be indicative of specific pathologies, typically involving either insufficient progesterone production by the corpus luteum, or impaired receptivity of the endometrium to progesterone resulting in early destabilization of the lining.
If you have a short luteal phase or labs show low progesterone (keep in mind that it’s key that progesterone labs are done 7 days post ovulation - not necessarily CD 21), it can be tempting to think that supplemental progesterone will fix the issue.
Progesterone supplementation can be helpful in early pregnancy if you do conceive and have a history of low progesterone, however simply supplementing with progesterone will not have any effect on follicle, egg, or corpus luteum development in cycles when you’re trying to conceive.
It’s also important to note that if you begin taking progesterone too early — for example before you ovulate, based on the assumption that you’re ovulating on a certain day, but without confirming ovulation has actually occurred — you will likely delay or suppress ovulation.
To truly improve your progesterone production, the focus must be on improving follicle and egg development in the first half of the cycle by ruling out and identifying the specific factors impacting your hormone cycle.
Timelines of Events
Follicular Phase:
In the Uterus:
On Cycle Day 1, your endometrium begins to shed in response to the disintegration of the corpus luteum and the subsequent withdrawal of progesterone resulting in destabilization of the endometrium (uterine lining) and a subsequent period.
In the Ovary:
A handful of follicles have been recruited to attempt ovulation this cycle - recruitment of these follicles started 3 to 4 months prior - we call this the Critical 90 Days of Egg Development.
Follicles are fluid filled sacs within the ovary that each contain an immature egg
An immature egg is one that has been halted in the early stage of meiosis (pronounced: my-oh-sis) which began when you were developing as a fetus in your own mother’s womb. Before your birth, this process was paused until puberty when your first wave of follicles was recruited to begin development in preparation for your first ovulation.
Meiosis is the process of cell division that reduces the number of parent chromosomes contained within the egg cell from the 46 (identical to the copies you carry in all of your cells) to the 23 that will be passed on to your future baby.
Follicles play a crucial role in the development of the mature egg by regulating the process of meiosis and providing the nutrients and energy needed to carry out this critical genetic division precisely.
In the Brain:
The hypothalamus begins to release GnRH (Gonadotropin Releasing Hormone) to stimulate the pituitary to release FSH (Follicle Stimulating Hormone) into the blood stream.
FSH reaches receptors on the ovarian follicles and induces them to begin growing and activating the maturation of the egg cells - aka resuming meiosis.
As the follicles grow in response to the FSH, they produce estrogen and release it into the blood stream.
Effects of Estrogen:
On the uterus:
Estrogen travels through the blood stream to bind with receptors within the uterine lining and induces the endometrium to begin growing and thickening.
On the brain:
At low levels, while there are several small follicles growing and producing estrogen, estrogen stimulates the pituitary to increase FSH production and release to continue promoting follicular growth.
At peak levels, reached when a dominant follicle has taken the lead and outgrown all of the other follicles (which then disintegrate and are reabsorbed), estrogen signals the pituitary to stop making FSH and to release a surge of LH (Luteinizing Hormone)
The dominant follicle is the one that has more FSH receptors than the other developing follicles and can therefore respond more quickly to its effects
Luteinizing Hormone:
Is released from the pituitary in response to peak estrogen levels.
Acts on the dominant follicle to trigger the final stages of chromosomal division that allow for fertilization.
Weakens the follicular wall to allow the mature egg to emerge from the follicle - the actual process that we call ovulation.
Initiates the transformation of the follicle into the progesterone producing corpus luteum.
Ovulation:
The egg is released from the ovarian follicle into the pelvic cavity where it is gathered up by the fimbrils of the fallopian tube.
It is within the fallopian tube that fertilization will occur if sperm are present and the egg and sperm are both genetically sound.
If fertilization does occur, it takes about 5-8 days for the developing embryo to travel through the fallopian tube to the uterine cavity
The Luteal Phase:
In the follicle:
Following ovulation, as a result of the LH surge, the cells of the vacated follicle undergo structural and functional changes to shift from primarily producing estrogen to producing large amounts of progesterone.
This restructured follicle is called the corpus luteum.
The corpus luteum is the source all of the progesterone necessary to stabilize the endometrium in preparation for implantation and to sustain early pregnancy prior to the formation of a placenta (at approximately 10 weeks gestation)
Progesterone:
Effects on Uterus:
Progesterone travels from the corpus luteum through the blood stream to the uterus to counteract the effects of estrogen on the endometrium.
Under the influence of progesterone, the endometrium stops growing, becomes increasingly vascularized, and begins secreting nutrients to support embryo implantation and growth.
Progesterone reduces the number of estrogen receptors on the endometrium and promotes estrogen metabolism.
Additionally, progesterone influences immune activity in the endometrium to increase tolerance of the embryo and reducing inflammation that may impact implantation.
In the absence of conception/ implantation of a viable embryo
The corpus luteum breaks down and stops producing progesterone after 14 days.
Dropping progesterone levels cause the endometrium to destabilize, allowing it to be shed as the next period.